At Children’s Memorial Hermann Hospital, our multidisciplinary team approach combines affiliated fetal cardiologists from The Fetal Cardiology Program at The Fetal Center with the affiliated, pediatric heart specialists at the Children’s Heart Institute to deliver comprehensive, quality care for patients with Tetralogy of Fallot before, during and after birth.
What Is Tetralogy of Fallot?
Tetralogy of Fallot (TOF) is a complex, congenital (present at birth) heart condition involving four related heart defects that commonly occur together. While serious, these defects are surgically correctable, which enables a positive outcome for most children.
A normal heart has four chambers: the right atrium and ventricle and the left atrium and ventricle. It also has four valves (tissue flaps) that are vital to the heart’s normal function and keep blood flowing in a forward direction. With each heartbeat, the valves in the heart open and shut with contraction and relaxation of the heart’s chambers to propel blood through the heart and to the rest of the body."
TOF’s four heart defects include:
- Ventricular septal defect or VSD: a hole exists in the wall between the heart’s main pumping chambers (ventricles).
- Pulmonary stenosis or PS: the valve between the heart and lungs (pulmonary valve) is narrow or stiff and blocks normal blood flow from the ventricle to the lungs.
- Right ventricular hypertrophy: the right ventricle’s muscular walls become thick due to the extra work it takes to pump blood through the narrowed pulmonary valve.
- Overriding aorta: the aorta, the main blood vessel leading from the heart to the body, is shifted over in the wrong location, generally above both the right and left ventricles instead of just above the left ventricle (as in healthy hearts).
TOF’s name comes from Etienne-Louis Arthur Fallot (fah-LO), the doctor who first described this combination of heart defects and named them a “tetralogy.”
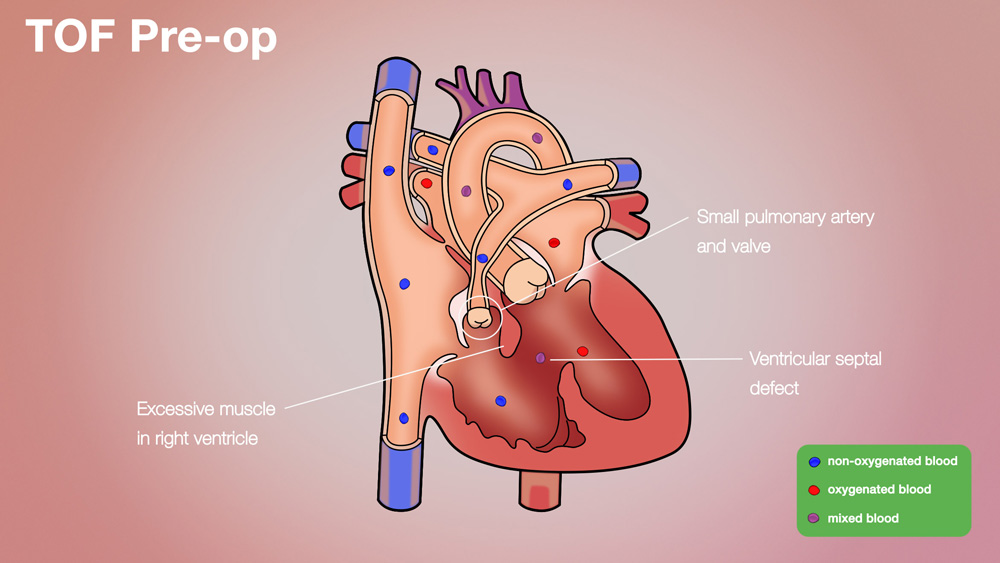
Tetralogy of Fallot (TOF) Pre-op
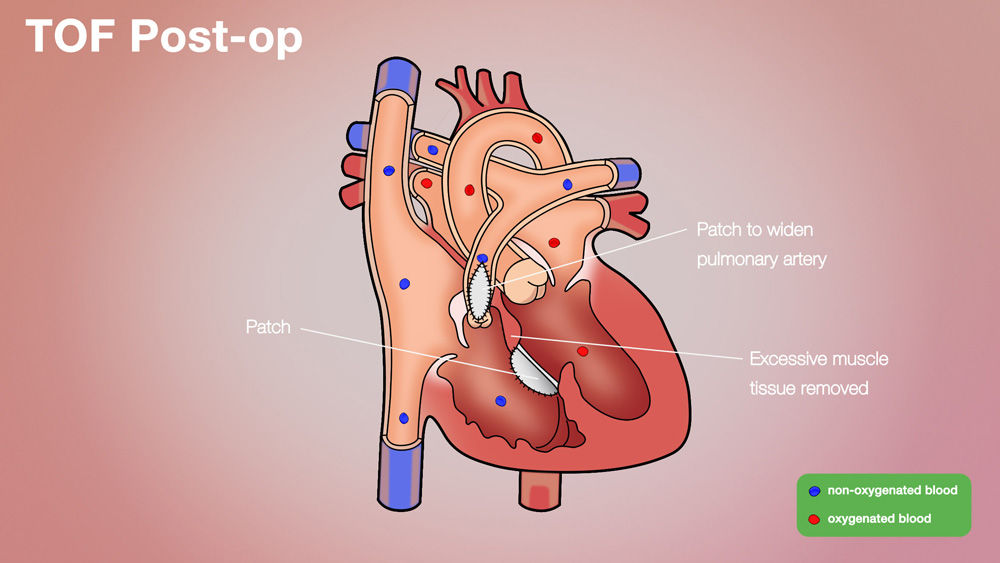
Tetralogy of Fallot (TOF) Post-op
What Are the Causes?
The exact causes of TOF are unknown, though genes may contribute. Genetic syndromes, including Down syndrome, Alagille syndrome and DiGeorge syndrome (also known as 22q11 deletion syndrome) may be associated with TOF. The condition also can be linked to cleft and palate abnormalities.
How Is It Diagnosed?
TOF may be diagnosed during pregnancy with a fetal echocardiogram, which is a specialized ultrasound of the fetal heart. The affiliated physicians in the Fetal Cardiology Program at The Fetal Center will confirm a diagnosis and prepare a delivery plan for both mom and baby. A multidisciplinary team of specialists will also develop the baby's immediate care plan following delivery.
If TOF is not diagnosed in utero, and suspicion of a heart defect occurs after the baby is born, a pediatrician will refer the patient to a pediatric cardiologist or neonatologist to determine the diagnosis.
There are two types of TOF. Some children are considered “Pink” tets, while others may be considered “Blue” tets. This designation is based upon the amount of pulmonary stenosis and the degree of restriction of blood flow to the lungs. One of the first signs of a blue TOF might be a blue tint (cyanosis) to an infant’s lips, skin and nails. Seek prompt medical attention should a baby become deep blue colored or struggle to breathe and cry. This is known as hypercyanotic episodes or tet spells.
Doctors may hear a heart murmur (or whooshing sound) via stethoscope during a routine baby check. TOF babies also might become fussy, lethargic or fail to gain weight.
The following tests may be utilized to find more details:
- An echocardiogram (ECHO) uses sound waves (ultrasound) to produce images on a screen of the heart and blood vessels in action that reveals whether the heart is pumping properly.
- An electrocardiogram (EKG or ECG), a painless exam, checks the heart’s electrical activity to reveal chamber enlargement, damage or irregular rhythms, suggesting a struggling right ventricle.
- Pulse oximetry, a small and painless gadget placed on a finger, may reveal a low oxygen level in the blood. In TOF, oxygen levels may be lower than normal.
- Chest X-rays create images of the heart and lungs, and major defects will be visible.
- A cardiac MRI (magnetic resonance imaging) uses radio waves, magnets and a computer to form images of the heart, which can reveal structural abnormalities.
- Cardiac catheterization involves a thin, long tube that is inserted into a blood vessel and guided into an artery or vein in the heart. The doctor can widen narrowed vessels at that time, to improve blood oxygen levels short-term.
How Is It Treated?
Unless there is some unusual complicating factor, all children with TOF should undergo surgical correction. Even those with mild symptoms will do better in the long run with corrective surgery than if left alone. Surgery is an open-heart surgery, done using an up-and-down (vertical) incision in the midline of the chest. It is necessary to place patients on the heart-lung machine during surgery. Tubes are placed in the vessels coming back to the heart to draw blood away before it gets to the heart. The machine oxygenates the blood and pumps it back into the body. In this way, the surgeon can work inside the heart more easily. Surgery involves closure of the hole in the wall (ventricular septal defect) between the heart’s ventricles using a patch, and opening the narrowed artery to the lungs. The technique used to open the artery will vary, depending upon severity of the narrowing. The child is then weaned off of the heart-lung machine, the heart and lungs are allowed to take over the work of supplying oxygenated blood to the body, the chest is closed and the operation is completed.
If the child is too small or ill for complete repair, a temporary repair can be performed, to boost the amount of blood reaching the lungs and raise blood oxygen levels. This occurs by surgical placement of a Blalock-Taussig (BT) shunt, in which a tube is placed to connect an artery from the left side to the pulmonary arteries so lungs will receive more blood. Such temporary surgery will help until the baby is ready for the definitive surgical correction.
What Are the Long-Term Effects?
Most children stay in the hospital from 4-10 days after repair of TOF. Children often leave the hospital on some medications, but these can usually be discontinued within a couple of months after surgery.
Most children do very well for many years after surgery for TOF. However, the surgery cannot be considered a true “cure.” In normal hearts, there are usually two valves on the right side of the heart. (A valve keeps blood going in the correct direction.) Most children have only one valve on the right side after surgery for TOF. Usually, this does not cause any problems. In some, however, the right side of the heart may become overburdened because of this and may need another operation years after the original repair. This only happens to a few percent of the children, but it is important to make sure that all children who have TOF are followed regularly by a cardiologist.
Why Choose the Children’s Heart Institute?
At Children’s Heart Institute at Children’s Memorial Hermann Hospital, patients with congenital or acquired heart disorders receive hands-on specialized care 24/7 from a team of affiliated physicians and specialty-trained nurses who aim to deliver the best possible outcomes.
Children’s Memorial Hermann Hospital was named one of the top children's hospitals nationally in Cardiology & Heart Surgery by U.S. News & World Report. In addition, Children’s Heart Institute is among the top congenital heart surgery programs in North America for patient care and outcomes, according to the Fall 2019 Society of Thoracic Surgeons (STS) Congenital Heart Surgery Database Report of 118 STS participating programs.
In collaboration with various subspecialties, the affiliated team provides comprehensive care for newborns, children and adolescents, with the ability to transition into adult congenital cardiac care. Team members have the experience and skills necessary to offer innovative treatment methods and specialized services, including, but not limited to:
- Biventricular repairs and biventricular conversions
- Congenital heart optimization
- Full repairs for complex congenital heart defects in newborns
- Hybrid catheterization and surgical procedures
- Minimally invasive transcatheter pulmonary valve (TPV) therapy
- Minimally invasive repairs
- Treatment for adult congenital heart disease
- Valve repairs and preservation
With the Level IV Neonatal Intensive Care Unit (NICU) and a dedicated Children’s Heart Institute Intensive Care Unit at Children’s Memorial Hermann Hospital, critical heart patients have access to quality, specialized care. By utilizing state-of-the-art techniques, the team at Children’s Heart Institute strives to offer patients with the most complex problems the greatest opportunity for a normal life.
Contact Us
If you have any questions, use the online tool below to help us connect with you. To refer a patient or schedule an appointment, please contact our clinic using the information below.
- Pediatric Cardiology Clinic
The University of Texas Health Science Center Professional Building
6410 Fannin, Suite 370
Houston, TX 77030
Phone: (713) 486-6755 (Appointment Line)
- Pediatric and Congenital Heart Surgery Clinic
The University of Texas Health Science Center Professional Building
6410 Fannin, Suite 370
Houston, TX 77030
Phone: (713) 500-5746
CMHH-Heart@memorialhermann.org
To contact Children's Memorial Hermann Hospital, please fill out the form below.
The Children’s Heart Institute is a collaboration between the affiliated physicians at McGovern Medical School at UTHealth Houston and Children’s Memorial Hermann Hospital. Typically, patients are seen on an outpatient basis at a UT Physicians clinic with all inpatient procedures performed at Children’s Memorial Hermann Hospital.
Nationally Ranked Pediatric Care
Proud to be named one of the nation’s best in Cardiology and Heart Surgery; Gastroenterology and GI Surgery; Neonatology; and Neurology and Neurosurgery.
Learn More