What Is Gastroschisis?

Gastroschisis occurs in approximately one in every 2,000 live births and the incidence appears to be increasing.
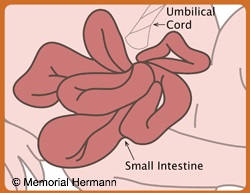
In mild cases, only small portions of intestine are outside of the abdomen. Most of the organs develop normally. In some cases, portions of the intestine can develop improperly. Because the bowel is free to float in the amniotic fluid, the intestines can twist and develop kinks, blockages, or separations. When this happens, the infant can be born with only a short segment of working bowel. This can be a significant problem that can only be determined after birth. Your pediatric surgeon will discuss these issues if they are suspected.
Gastroschisis Prenatal Care Algorithm PDF
The cause of gastroschisis is unknown. This condition does not run in families. Most infants with gastroschisis do not have chromosomal or genetic syndromes, but sometimes may result in low birthweight, preterm delivery, and stillbirth. Although both are abdominal wall defects, gastroschisis differs significantly from an omphalocele. Please see omphalocele to learn these differences.
What Will Happen During Pregnancy?
Gastroschisis can be detected by ultrasound from about the third month of pregnancy. Once the condition has been detected, a series of ultrasounds will be performed throughout pregnancy to evaluate the fetal bowel and to assess fetal growth. Sometimes a specialized ultrasound of the fetal heart, called an echocardiogram, will be performed. Antenatal testing is usually initiated in the third trimester.
Will a Fetal Treatment Be Required?
There is no fetal intervention available for gastroschisis.
What Special Considerations Should Be Made for Delivery?
Type of Delivery: Gastroschisis does not always require cesarean delivery. The delivery plan should be carefully discussed between the mother and her obstetrician.
Place of Delivery: The baby should be delivered at a hospital that is well prepared to handle the intensive care and surgery required of infants with gastroschisis. There should be a neonatal intensive care unit with the capability to provide specialized care and pediatric surgery services.
Time of Delivery: There is usually no reason for early delivery of babies with gastroschisis. Babies will benefit from being allowed to reach full gestational maturity, if possible. Sometimes early delivery is recommended if the baby is not growing well inside the uterus.
What Will Happen at Birth?
Immediately following delivery, doctors will carefully evaluate the baby and start treatment. After a brief period with mom and family, the baby will be transferred to the neonatal intensive care unit. A pediatric surgeon will see and evaluate your baby. The baby will be stabilized in an intensive care unit and, depending on the size of the hole in the abdominal wall a protective pouch (silo) may be placed over the exposed intestines and/or organs to protect them from infection and/or damage.
What Will Happen After Delivery?
After the gastroschisis is repaired, it may be several weeks before the baby’s intestinal tract functions normally. Because the intestines have been very swollen and inflamed, the intestines will not be ready to handle food immediately. Before any attempts at feeding, the baby must show that proper GI function has returned. In the meantime, the baby will be provided IV nutrition through total parenteral nutrition (TPN).
What Are the Long-Term Outcomes and Considerations?
In almost all cases of gastroschisis, the long-term prognosis is excellent. Most babies will recover to lead a normal life with no complications. Some babies with gastroschisis will be born with a blockage or atresia which would require additional surgery. In a small percentage of cases, babies experience prolonged intestinal problems and some may have issues with bowel function especially those that have a short amount of intestine. If this occurs, your doctors will discuss the long-term plans in caring for your child.

Cassandra's Story: Gastroschisis
As Sabrina sat at her 16-week checkup, she was expecting her appointment to be ordinary. However, after receiving her ultrasound, she found out her baby girl was diagnosed with a birth defect known as...
Read MoreContact Us
When you contact The Fetal Center, you will be in touch with a dedicated coordinator who will walk you through the process step-by-step and help you to understand every aspect of your care.
The Fetal Center at Children's Memorial Hermann Hospital
UT Professional Building
6410 Fannin, Suite 210
Houston, Texas 77030
Phone: (832) 325-7288
Toll free: (888) 818-4818
Fax: (713) 383-1464
Email: thefetalcenter@memorialhermann.org
To contact The Fetal Center at Children's Memorial Hermann Hospital, please fill out the form below.
Located within the Texas Medical Center, The Fetal Center is affiliated with McGovern Medical School at UTHealth Houston, UT Physicians and Children’s Memorial Hermann Hospital.